
article_id
stringlengths 6
7
| url
stringlengths 19
20
| article_data
listlengths 1
7
| questions
listlengths 0
5
|
|---|---|---|---|
937560 | /viewarticle/937560 | [
{
"authors": "Jeffrey S. Forrest, MD; Alexander B. Shortridge",
"content": [
"Editor's Note: The Case Challenge series includes difficult-to-diagnose conditions, some of which are not frequently encountered by most clinicians, but are nonetheless important to accurately recognize. Test your diagnostic and treatment skills using the following patient scenario and corresponding questions. If you have a case that you would like to suggest for a future Case Challenge, please email us at [email protected] with the subject line \"Case Challenge Suggestion.\" We look forward to hearing from you.",
"A 36-year-old man is brought to the emergency department on a temporary detention order (involuntary hold) after an evaluation by the municipal crisis assessment team. The patient had been extremely upset during a disagreement with his significant other. He had become disproportionately enraged and proceeded to yell, throw possessions, and break his phone. He then used a razor blade to make numerous superficial slashes on the inside of both of his forearms. At that point, his concerned adoptive parents called the behavioral health crisis unit.",
"During his intake evaluation, the patient reports that he has injured himself on many prior occasions, including punching himself and using a cigarette lighter to burn himself on various places on his body. When asked what made him upset enough to want to do these things, the patient states, \"Everyone hates me, they always leave me!\" He then becomes hostile toward the evaluator and says, \"The other intake counselor was much better than you. People like you are the reason I want to hurt myself!\" A brief review of hospital records reveals that the patient has had multiple similar presentations over the past several years.",
"On follow-up evaluation, the patient reveals that conflicts in his personal relationships are commonplace. He says, \"I don't even know who I am anymore. People are all just using me.\" The patient states that he is frequently reckless in his behavior, explaining, \"Sometimes I go out and hook up with people on dating apps just to feel something. I always just feel empty afterward.\"",
"The patient acknowledges occasionally starving himself when he is not having a good day. He has significantly unstable moods. He explains, \"Some days, it feels like everything is awesome, but within a few hours or a day I wake up and realize that it all just sucks.\" When asked how long this has been going on, he says, \"I've always been this way.\"",
"The patient has occasional difficulty in getting to sleep; however, he states that he always feels the need and desire to sleep, he is simply unable to do so at times. When asked whether he ever attempted suicide before, he recounts, \"One time I took 10 ibuprofen pills to show my parents how hateful they are.\" The patient denies current plans or intentions for suicidal action but states, \"Sometimes I get tired and just don't want to feel anything anymore. It's always hot or cold, there's nothing ever in the middle.\" When asked about his parents and his significant other, he says, \"I would not actually hurt them, but I hope they feel bad when I cut myself.\""
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# A Distraught Man Engaging in Self-Injury\n\n **Authors:** Jeffrey S. Forrest, MD; Alexander B. Shortridge \n **Date:** February 07, 2025\n\n ## Content\n\n Editor's Note: The Case Challenge series includes difficult-to-diagnose conditions, some of which are not frequently encountered by most clinicians, but are nonetheless important to accurately recognize. Test your diagnostic and treatment skills using the following patient scenario and corresponding questions. If you have a case that you would like to suggest for a future Case Challenge, please email us at [email protected] with the subject line \"Case Challenge Suggestion.\" We look forward to hearing from you.\nA 36-year-old man is brought to the emergency department on a temporary detention order (involuntary hold) after an evaluation by the municipal crisis assessment team. The patient had been extremely upset during a disagreement with his significant other. He had become disproportionately enraged and proceeded to yell, throw possessions, and break his phone. He then used a razor blade to make numerous superficial slashes on the inside of both of his forearms. At that point, his concerned adoptive parents called the behavioral health crisis unit.\nDuring his intake evaluation, the patient reports that he has injured himself on many prior occasions, including punching himself and using a cigarette lighter to burn himself on various places on his body. When asked what made him upset enough to want to do these things, the patient states, \"Everyone hates me, they always leave me!\" He then becomes hostile toward the evaluator and says, \"The other intake counselor was much better than you. People like you are the reason I want to hurt myself!\" A brief review of hospital records reveals that the patient has had multiple similar presentations over the past several years.\nOn follow-up evaluation, the patient reveals that conflicts in his personal relationships are commonplace. He says, \"I don't even know who I am anymore. People are all just using me.\" The patient states that he is frequently reckless in his behavior, explaining, \"Sometimes I go out and hook up with people on dating apps just to feel something. I always just feel empty afterward.\"\nThe patient acknowledges occasionally starving himself when he is not having a good day. He has significantly unstable moods. He explains, \"Some days, it feels like everything is awesome, but within a few hours or a day I wake up and realize that it all just sucks.\" When asked how long this has been going on, he says, \"I've always been this way.\"\nThe patient has occasional difficulty in getting to sleep; however, he states that he always feels the need and desire to sleep, he is simply unable to do so at times. When asked whether he ever attempted suicide before, he recounts, \"One time I took 10 ibuprofen pills to show my parents how hateful they are.\" The patient denies current plans or intentions for suicidal action but states, \"Sometimes I get tired and just don't want to feel anything anymore. It's always hot or cold, there's nothing ever in the middle.\" When asked about his parents and his significant other, he says, \"I would not actually hurt them, but I hope they feel bad when I cut myself.\"\n\n ## Figures\n\n \n*Page 1 of 6*",
"pagination": {
"current_page": 1,
"total_pages": 6
},
"questionnaire": [],
"title": "A Distraught Man Engaging in Self-Injury"
},
{
"authors": "Jeffrey S. Forrest, MD; Alexander B. Shortridge",
"content": [
"The patient is 5 ft 7 in (1.7 m) and weighs 160 lb (72.57 kg). His blood pressure is 138/94 mm Hg, and his temperature is 98.3°F (36.8°C). His oxygen saturation is 97% on room air.",
"The patient appears disheveled and agitated, has tense posture, and exhibits increased psychomotor activity. An ecchymosis is noted on the right side of his forehead. Scarring and recent superficial cutting wounds are present on both forearms. An example of wounds similar to the patient's is shown in the figure below.",
"Figure 1.",
"The patient's heart rate is tachycardic at 110 beats/min. No murmurs, rubs, or gallops are audible. His heart rhythm is regular. His respiration rate is elevated at 18 breaths/min. His lungs are clear to auscultation bilaterally. His abdomen is nontender and tympanitic to percussion, with normal bowel sounds. He does not display facial droop, and his cranial nerves are otherwise intact.",
"During the mental status examination, the patient is alert and oriented to name, location, date, and time. He appears depressed and anxious and exhibits some motor overflow. His speech widely varies in volume, rhythm, and tone and fluctuates throughout the interview. His recall is good when measured for immediate, recent, and distant memory.",
"The patient's thought process is occasionally tangential, but he is able to be redirected. His thought content is dominated by current stressors. He keeps repeating, \"It's not fair.\" As noted in an earlier examination, the patient reports depression and a significant history of self-mutilating behaviors. When asked about his mood, he says, \"I feel empty.\" His affect is labile. He appears capable of attending to the interview but does not always cooperate. His insight is limited to poor, as he appears to downplay the significance of his behaviors. His judgment is similarly poor. The patient denies auditory and visual hallucinations.",
"An ECG shows a heart rate of 110 beats/min, but the findings are otherwise normal. A CT scan of the head without contrast reveals normal findings, with no evidence of a cerebrovascular accident, mass lesion, or bleeding. Urine toxicology screen results are negative. Urinalysis findings are within normal limits. His complete blood cell count, comprehensive metabolic profile, and thyroid-stimulating hormone levels are all within reference-range values."
],
"date": "February 07, 2025",
"figures": [
{
"caption": "Figure 1.",
"image_url": "https://img.medscapestatic.com/article/937/560/937560-Thumb1.jpg"
}
],
"markdown": "# A Distraught Man Engaging in Self-Injury\n\n **Authors:** Jeffrey S. Forrest, MD; Alexander B. Shortridge \n **Date:** February 07, 2025\n\n ## Content\n\n The patient is 5 ft 7 in (1.7 m) and weighs 160 lb (72.57 kg). His blood pressure is 138/94 mm Hg, and his temperature is 98.3°F (36.8°C). His oxygen saturation is 97% on room air.\nThe patient appears disheveled and agitated, has tense posture, and exhibits increased psychomotor activity. An ecchymosis is noted on the right side of his forehead. Scarring and recent superficial cutting wounds are present on both forearms. An example of wounds similar to the patient's is shown in the figure below.\nFigure 1.\nThe patient's heart rate is tachycardic at 110 beats/min. No murmurs, rubs, or gallops are audible. His heart rhythm is regular. His respiration rate is elevated at 18 breaths/min. His lungs are clear to auscultation bilaterally. His abdomen is nontender and tympanitic to percussion, with normal bowel sounds. He does not display facial droop, and his cranial nerves are otherwise intact.\nDuring the mental status examination, the patient is alert and oriented to name, location, date, and time. He appears depressed and anxious and exhibits some motor overflow. His speech widely varies in volume, rhythm, and tone and fluctuates throughout the interview. His recall is good when measured for immediate, recent, and distant memory.\nThe patient's thought process is occasionally tangential, but he is able to be redirected. His thought content is dominated by current stressors. He keeps repeating, \"It's not fair.\" As noted in an earlier examination, the patient reports depression and a significant history of self-mutilating behaviors. When asked about his mood, he says, \"I feel empty.\" His affect is labile. He appears capable of attending to the interview but does not always cooperate. His insight is limited to poor, as he appears to downplay the significance of his behaviors. His judgment is similarly poor. The patient denies auditory and visual hallucinations.\nAn ECG shows a heart rate of 110 beats/min, but the findings are otherwise normal. A CT scan of the head without contrast reveals normal findings, with no evidence of a cerebrovascular accident, mass lesion, or bleeding. Urine toxicology screen results are negative. Urinalysis findings are within normal limits. His complete blood cell count, comprehensive metabolic profile, and thyroid-stimulating hormone levels are all within reference-range values.\n\n ## Figures\n\n **Figure 1.** \n \n\n\n*Page 2 of 6*",
"pagination": {
"current_page": 2,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1526219,
"choiceText": "Bipolar disorder",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526220,
"choiceText": "Adjustment disorder",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526221,
"choiceText": "Histrionic personality disorder",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526222,
"choiceText": "Borderline personality disorder",
"correct": true,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526223,
"choiceText": "Posttraumatic stress disorder",
"correct": false,
"displayOrder": 5,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 489044,
"questionText": "Based only on these findings, which of the following is the most likely diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "A Distraught Man Engaging in Self-Injury"
},
{
"authors": "Jeffrey S. Forrest, MD; Alexander B. Shortridge",
"content": [
"This patient's presentation and reported history most strongly correlate with a diagnosis of borderline personality disorder (BPD). BPD is a pervasive pattern of behavior characterized by unstable interpersonal relationships, self-image, and affect, as well as impulsive self-harming behavior.[1] The term \"borderline personality\" was first coined by Adolph Stern in 1938 to describe his patients who \"bordered\" between psychosis and neurosis.[2]",
"According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5-TR), a diagnosis of BPD requires the presence of five or more of the following personality characteristics[1]:",
"Frantic efforts to avoid real or imagined abandonment",
"A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization (in which a person assigns exaggeratedly positive characteristics to the self or others) and devaluation (in which a person assigns exaggeratedly negative characteristics to the self or others), commonly referred to as \"splitting\"[3]",
"Identity disturbance, with a markedly and persistently unstable self-image or sense of self",
"Impulsivity in at least two areas that are potentially self-damaging (eg, spending, sex, substance abuse, reckless driving, binge eating)",
"Recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior",
"Affective instability due to a marked reactivity of mood (eg, intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days)",
"Chronic feelings of emptiness",
"Inappropriate, intense anger or difficulty in controlling anger (eg, frequent displays of temper, constant anger, recurrent physical fights)",
"Transient, stress-related paranoid ideation or severe dissociative symptoms",
"The lifetime prevalence of BPD in a US community sample was 2.7% (3% for women vs 2.4% for men)[4]; the American Psychiatric Association cites a lifetime prevalence of BPD in the United States as 1.4% - 2.7%.[18] In psychiatric settings, this estimate is about 15% to 28%.[5] Data from family studies have demonstrated that the prevalence of BPD among first-degree relatives of affected patients is 4- to 20-fold higher than in the general population.[6]",
"The ways in which BPD personality patterns are generated are diverse and multifactorial. Environmental factors have been identified in BPD pathogenesis, including childhood maltreatment, adoption, maternal separation, poor maternal attachment, inappropriate family boundaries, parental substance abuse, and serious parental psychopathology.[7] Posttraumat/sup>ic stress disorder and BPD can co-occur.",
"Certain genetic factors may also play a role in the onset of BPD. Data from twin studies show that the heritability of BPD is approximately 40%..[7] Of note, these same studies found a higher concordance of BPD for monozygotic than for dizygotic twins. Alterations in the social reward and empathy networks of the brain caused by dysregulation of the oxytocinergic system may contribute to BPD pathology.[8]"
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# A Distraught Man Engaging in Self-Injury\n\n **Authors:** Jeffrey S. Forrest, MD; Alexander B. Shortridge \n **Date:** February 07, 2025\n\n ## Content\n\n This patient's presentation and reported history most strongly correlate with a diagnosis of borderline personality disorder (BPD). BPD is a pervasive pattern of behavior characterized by unstable interpersonal relationships, self-image, and affect, as well as impulsive self-harming behavior.[1] The term \"borderline personality\" was first coined by Adolph Stern in 1938 to describe his patients who \"bordered\" between psychosis and neurosis.[2]\nAccording to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5-TR), a diagnosis of BPD requires the presence of five or more of the following personality characteristics[1]:\nFrantic efforts to avoid real or imagined abandonment\nA pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization (in which a person assigns exaggeratedly positive characteristics to the self or others) and devaluation (in which a person assigns exaggeratedly negative characteristics to the self or others), commonly referred to as \"splitting\"[3]\nIdentity disturbance, with a markedly and persistently unstable self-image or sense of self\nImpulsivity in at least two areas that are potentially self-damaging (eg, spending, sex, substance abuse, reckless driving, binge eating)\nRecurrent suicidal behavior, gestures, or threats, or self-mutilating behavior\nAffective instability due to a marked reactivity of mood (eg, intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days)\nChronic feelings of emptiness\nInappropriate, intense anger or difficulty in controlling anger (eg, frequent displays of temper, constant anger, recurrent physical fights)\nTransient, stress-related paranoid ideation or severe dissociative symptoms\nThe lifetime prevalence of BPD in a US community sample was 2.7% (3% for women vs 2.4% for men)[4]; the American Psychiatric Association cites a lifetime prevalence of BPD in the United States as 1.4% - 2.7%.[18] In psychiatric settings, this estimate is about 15% to 28%.[5] Data from family studies have demonstrated that the prevalence of BPD among first-degree relatives of affected patients is 4- to 20-fold higher than in the general population.[6]\nThe ways in which BPD personality patterns are generated are diverse and multifactorial. Environmental factors have been identified in BPD pathogenesis, including childhood maltreatment, adoption, maternal separation, poor maternal attachment, inappropriate family boundaries, parental substance abuse, and serious parental psychopathology.[7] Posttraumat/sup>ic stress disorder and BPD can co-occur.\nCertain genetic factors may also play a role in the onset of BPD. Data from twin studies show that the heritability of BPD is approximately 40%..[7] Of note, these same studies found a higher concordance of BPD for monozygotic than for dizygotic twins. Alterations in the social reward and empathy networks of the brain caused by dysregulation of the oxytocinergic system may contribute to BPD pathology.[8]\n\n ## Figures\n\n \n*Page 3 of 6*",
"pagination": {
"current_page": 3,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1526219,
"choiceText": "Bipolar disorder",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526220,
"choiceText": "Adjustment disorder",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526221,
"choiceText": "Histrionic personality disorder",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526222,
"choiceText": "Borderline personality disorder",
"correct": true,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526223,
"choiceText": "Posttraumatic stress disorder",
"correct": false,
"displayOrder": 5,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 489044,
"questionText": "Based only on these findings, which of the following is the most likely diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "A Distraught Man Engaging in Self-Injury"
},
{
"authors": "Jeffrey S. Forrest, MD; Alexander B. Shortridge",
"content": [
"Environmental factors have been identified in BPD pathogenesis, including childhood maltreatment, adoption, maternal separation, poor maternal attachment, inappropriate family boundaries, parental substance abuse, and serious parental psychopathology.[7]",
"Data from twin studies show that the heritability of BPD is approximately 40%.%.[7]",
"Posttraumatic stress disorder and BPD can co-occur.",
"The lifetime prevalence of BPD in a US community sample was 2.7% (3% for women vs 2.4% for men).[4]",
"Clinicians should be aware of the current frameworks used to diagnose BPD. The DSM-5 utilizes two models of diagnosis: categorical and dimensional.[9] BPD is conventionally diagnosed using a categorical model (ie, a patient either does or does not receive a diagnosis by meeting specified criteria).[10] A dimensional model of diagnosis characterizes a condition based on a spectrum of prominent traits.[9] Given that five of the nine DSM-5 criteria must be met to receive a diagnosis by the current categorical standard, presentations may vary significantly among patients described as having the same condition. To address this variation, the categorical approach is often used in conjunction with a dimensional approach.[10]",
"One approach that may prove useful in performing a dimensional diagnosis of BPD is the Five Factor Model. The Five Factor Model describes personality on a continuum based on five characteristics: neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness.[11] It has been demonstrated that BPD can be differentiated from other personality disorders based on specific differences in Five Factor Model traits.[12]",
"Although BPD shares many characteristics with bipolar affective disorders, they are entirely distinct diagnostic entities. Both conditions may involve dramatic shifts in mood; however, the timing, duration, intensity, and pattern of the mood shifts may be very different. BPD is characterized by affective instability: \"a marked reactivity of mood (eg, intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days).\"[1] Conversely, bipolar disorders feature episodes of affective extremes, high or low, that may last for days, weeks, or months. Patients with BPD typically shift from euthymia to anger, whereas patients with bipolar disorders tend to shift from depression to elation.[13] Although BPD and bipolar disorders are different conditions, it is possible for the two to occur concomitantly in the same individual.[14]",
"To further differentiate BPD from bipolar disorders, it is worth examining the sleep disturbances associated with both conditions. Patients with BPD experience sleep disturbances such as increased sleep-onset latency, low sleep efficiency, and nightmares.[15] In contrast, patients with bipolar disorders commonly experience a reduced need for sleep (not merely decreased sleep) during a manic episode and (excessive sleepiness (hypersomnia) during depressive episodes.[16] Note that the patient in this case stated that he always felt the need and desire to sleep, despite clearly having difficulty in sleeping.",
"Clinicians should be aware of the ego-syntonic nature of BPD behaviors. Personality disorders consist of ego-syntonic patterns of behavior.[17] This means that the problematic conduct exhibited is not inherently distressing to the person performing it.[1] The patterns may feel natural or even instinctive. Their personality is not ego-alien to them. However, it is important to make the distinction that the consequences of ego-syntonic behaviors may well become very distressing for such a patient, even if the performance of the behavior is not. In the case presented, the patient reports a history of frequent self-mutilation and casually endorses doing so as a regular coping mechanism. By contrast, mood disorders such as major depression or bipolar disorder are typically ego-dystonic[17]; the behaviors are, or ultimately become, inherently distressing to the person who exhibits them."
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# A Distraught Man Engaging in Self-Injury\n\n **Authors:** Jeffrey S. Forrest, MD; Alexander B. Shortridge \n **Date:** February 07, 2025\n\n ## Content\n\n Environmental factors have been identified in BPD pathogenesis, including childhood maltreatment, adoption, maternal separation, poor maternal attachment, inappropriate family boundaries, parental substance abuse, and serious parental psychopathology.[7]\nData from twin studies show that the heritability of BPD is approximately 40%.%.[7]\nPosttraumatic stress disorder and BPD can co-occur.\nThe lifetime prevalence of BPD in a US community sample was 2.7% (3% for women vs 2.4% for men).[4]\nClinicians should be aware of the current frameworks used to diagnose BPD. The DSM-5 utilizes two models of diagnosis: categorical and dimensional.[9] BPD is conventionally diagnosed using a categorical model (ie, a patient either does or does not receive a diagnosis by meeting specified criteria).[10] A dimensional model of diagnosis characterizes a condition based on a spectrum of prominent traits.[9] Given that five of the nine DSM-5 criteria must be met to receive a diagnosis by the current categorical standard, presentations may vary significantly among patients described as having the same condition. To address this variation, the categorical approach is often used in conjunction with a dimensional approach.[10]\nOne approach that may prove useful in performing a dimensional diagnosis of BPD is the Five Factor Model. The Five Factor Model describes personality on a continuum based on five characteristics: neuroticism, extraversion, openness to experience, agreeableness, and conscientiousness.[11] It has been demonstrated that BPD can be differentiated from other personality disorders based on specific differences in Five Factor Model traits.[12]\nAlthough BPD shares many characteristics with bipolar affective disorders, they are entirely distinct diagnostic entities. Both conditions may involve dramatic shifts in mood; however, the timing, duration, intensity, and pattern of the mood shifts may be very different. BPD is characterized by affective instability: \"a marked reactivity of mood (eg, intense episodic dysphoria, irritability, or anxiety usually lasting a few hours and only rarely more than a few days).\"[1] Conversely, bipolar disorders feature episodes of affective extremes, high or low, that may last for days, weeks, or months. Patients with BPD typically shift from euthymia to anger, whereas patients with bipolar disorders tend to shift from depression to elation.[13] Although BPD and bipolar disorders are different conditions, it is possible for the two to occur concomitantly in the same individual.[14]\nTo further differentiate BPD from bipolar disorders, it is worth examining the sleep disturbances associated with both conditions. Patients with BPD experience sleep disturbances such as increased sleep-onset latency, low sleep efficiency, and nightmares.[15] In contrast, patients with bipolar disorders commonly experience a reduced need for sleep (not merely decreased sleep) during a manic episode and (excessive sleepiness (hypersomnia) during depressive episodes.[16] Note that the patient in this case stated that he always felt the need and desire to sleep, despite clearly having difficulty in sleeping.\nClinicians should be aware of the ego-syntonic nature of BPD behaviors. Personality disorders consist of ego-syntonic patterns of behavior.[17] This means that the problematic conduct exhibited is not inherently distressing to the person performing it.[1] The patterns may feel natural or even instinctive. Their personality is not ego-alien to them. However, it is important to make the distinction that the consequences of ego-syntonic behaviors may well become very distressing for such a patient, even if the performance of the behavior is not. In the case presented, the patient reports a history of frequent self-mutilation and casually endorses doing so as a regular coping mechanism. By contrast, mood disorders such as major depression or bipolar disorder are typically ego-dystonic[17]; the behaviors are, or ultimately become, inherently distressing to the person who exhibits them.\n\n ## Figures\n\n \n*Page 4 of 6*",
"pagination": {
"current_page": 4,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914552,
"choiceText": "Genetic factors are the main factor in the onset of BPD.",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914553,
"choiceText": "Early environmental factors play a role in BPD pathogenesis.",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914554,
"choiceText": "BPD and posttraumatic stress disorder do not occur concomitantly.",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914555,
"choiceText": "BPD primarily affects males.",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 4,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620036,
"questionText": "Which of the following statements about BPD is correct?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "A Distraught Man Engaging in Self-Injury"
},
{
"authors": "Jeffrey S. Forrest, MD; Alexander B. Shortridge",
"content": [
"Personality disorders consist of ego-syntonic (not ego-dystonic) patterns of behavior.[17]",
"The consequences of ego-syntonic behaviors may well become very distressing for a patient with BPD, even if the performance of the behavior is not.[1]",
"The behaviors of mood disorders are, or ultimately become, inherently distressing to the person who exhibits them.[17]",
"BPD is typically treated with different forms of psychotherapy.[18] Although many approaches to treating BPD are recognized, most emphasize teaching patients to recognize what triggers their affective reactions. Patients are also encouraged to connect their actions with their thoughts and feelings.[18]",
"One frequently recommended approach is dialectical behavior therapy. Dialectical behavior therapy is a widely used and effective form of cognitive behavior therapy that targets suicidal and self-harm behaviors using eight treatment strategies[19,20]:",
"Dialectical strategies foster the patient's ability to accept reality as it is. Therapists might accomplish this through the use of myth and paradox, a focus on reality as constantly changing, nonresolution of ambiguity, and cognitive challenging and restructuring.",
"Problem-solving strategies support the patient's ability to recognize sources of distress and address them in an adaptive way.",
"Validation strategies utilize empathetic, nonjudgmental acceptance of the patient's condition.",
"Irreverent communication strategies call for the therapist to respond in a matter-of-fact, irreverent way to the patient's suicidal tendencies. Such strategies are in direct contrast to validation strategies.",
"Consultant strategies emphasize the therapist's role as a consultant to the patient directly and not as a consultant to other treatment professionals.",
"Capability enhancement strategies serve to keep patients engaged in acquiring and practicing skills required to cope with everyday life.",
"Relationship strategies emphasize building a strong patient-therapist relationship, addressing interpersonal problems with this relationship as they arise, and learning to apply these skills to other relationships in the patient's life.",
"Contingency strategies involve the therapist being up-front with the patient about what outcomes reasonably can be expected from therapy.",
"BPD may be treated adjunctively with medication when appropriate.[18,21] Although no medications have been approved by the US Food and Drug Administration to specifically treat BPD, a broad spectrum of pharmacologic agents can be used to address specific symptoms.",
"Among antidepressants, one review of randomized controlled trials found that sertraline was effective in decreasing symptoms of depression, hypersensitivity in interpersonal relationships, and obsession in patients with BPD.[21] Among mood stabilizers, topiramate and lamotrigine were shown to reduce anger in patients with BPD. In regard to antipsychotics, olanzapine was found to reduce anger, paranoia, anxiety, and interpersonal sensitivity in patients with BPD.[21]",
"Clinicians should note that treating BPD with medication has limitations. Whereas some patients with BPD may respond to various medications initially, few respond satisfactorily over an extended period.[18]Duration of pharmacologic treatment should be time limited and ongoing review should be performed.[18]",
"Although BPD is viewed as a lifelong condition, its prognosis widely varies. Diagnostic criteria and standards have changed over time, and presentations may vary widely among patients, so predicting outcomes with precision is difficult. Research has shown that a diagnosis of early-onset BPD is associated with poor functioning in adolescence.[22] Evidence also suggests that the course of adolescent-onset BPD is similar to that seen in adult populations.",
"The rate of suicide associated with BPD is estimated to range between 3% and 10%.[18] Many persons who qualify for a diagnosis of BPD likely either take their lives by suicide before presenting or go through life without ever coming to clinical attention. Nonetheless, evidence indicates that early diagnosis and intervention can improve patient outcomes.[22]",
"Comorbid substance use disorders are associated with an increased risk of suicide in patients with BPD. Substance dependence or abuse is commonly observed in patients with BPD. Higher rates of comorbid psychiatric disorders are also seen in patients with BPD, including mood disorders (particularly major depressive disorder), anxiety disorders, and eating disorders.[18]",
"After his evaluation, the patient in this case was referred to a social worker, who assisted him in engaging with an appropriate dialectical behavior therapist for longitudinal management of his condition. The patient was also provided with a psychiatric referral to assess for the appropriateness of medical intervention."
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# A Distraught Man Engaging in Self-Injury\n\n **Authors:** Jeffrey S. Forrest, MD; Alexander B. Shortridge \n **Date:** February 07, 2025\n\n ## Content\n\n Personality disorders consist of ego-syntonic (not ego-dystonic) patterns of behavior.[17]\nThe consequences of ego-syntonic behaviors may well become very distressing for a patient with BPD, even if the performance of the behavior is not.[1]\nThe behaviors of mood disorders are, or ultimately become, inherently distressing to the person who exhibits them.[17]\nBPD is typically treated with different forms of psychotherapy.[18] Although many approaches to treating BPD are recognized, most emphasize teaching patients to recognize what triggers their affective reactions. Patients are also encouraged to connect their actions with their thoughts and feelings.[18]\nOne frequently recommended approach is dialectical behavior therapy. Dialectical behavior therapy is a widely used and effective form of cognitive behavior therapy that targets suicidal and self-harm behaviors using eight treatment strategies[19,20]:\nDialectical strategies foster the patient's ability to accept reality as it is. Therapists might accomplish this through the use of myth and paradox, a focus on reality as constantly changing, nonresolution of ambiguity, and cognitive challenging and restructuring.\nProblem-solving strategies support the patient's ability to recognize sources of distress and address them in an adaptive way.\nValidation strategies utilize empathetic, nonjudgmental acceptance of the patient's condition.\nIrreverent communication strategies call for the therapist to respond in a matter-of-fact, irreverent way to the patient's suicidal tendencies. Such strategies are in direct contrast to validation strategies.\nConsultant strategies emphasize the therapist's role as a consultant to the patient directly and not as a consultant to other treatment professionals.\nCapability enhancement strategies serve to keep patients engaged in acquiring and practicing skills required to cope with everyday life.\nRelationship strategies emphasize building a strong patient-therapist relationship, addressing interpersonal problems with this relationship as they arise, and learning to apply these skills to other relationships in the patient's life.\nContingency strategies involve the therapist being up-front with the patient about what outcomes reasonably can be expected from therapy.\nBPD may be treated adjunctively with medication when appropriate.[18,21] Although no medications have been approved by the US Food and Drug Administration to specifically treat BPD, a broad spectrum of pharmacologic agents can be used to address specific symptoms.\nAmong antidepressants, one review of randomized controlled trials found that sertraline was effective in decreasing symptoms of depression, hypersensitivity in interpersonal relationships, and obsession in patients with BPD.[21] Among mood stabilizers, topiramate and lamotrigine were shown to reduce anger in patients with BPD. In regard to antipsychotics, olanzapine was found to reduce anger, paranoia, anxiety, and interpersonal sensitivity in patients with BPD.[21]\nClinicians should note that treating BPD with medication has limitations. Whereas some patients with BPD may respond to various medications initially, few respond satisfactorily over an extended period.[18]Duration of pharmacologic treatment should be time limited and ongoing review should be performed.[18]\nAlthough BPD is viewed as a lifelong condition, its prognosis widely varies. Diagnostic criteria and standards have changed over time, and presentations may vary widely among patients, so predicting outcomes with precision is difficult. Research has shown that a diagnosis of early-onset BPD is associated with poor functioning in adolescence.[22] Evidence also suggests that the course of adolescent-onset BPD is similar to that seen in adult populations.\nThe rate of suicide associated with BPD is estimated to range between 3% and 10%.[18] Many persons who qualify for a diagnosis of BPD likely either take their lives by suicide before presenting or go through life without ever coming to clinical attention. Nonetheless, evidence indicates that early diagnosis and intervention can improve patient outcomes.[22]\nComorbid substance use disorders are associated with an increased risk of suicide in patients with BPD. Substance dependence or abuse is commonly observed in patients with BPD. Higher rates of comorbid psychiatric disorders are also seen in patients with BPD, including mood disorders (particularly major depressive disorder), anxiety disorders, and eating disorders.[18]\nAfter his evaluation, the patient in this case was referred to a social worker, who assisted him in engaging with an appropriate dialectical behavior therapist for longitudinal management of his condition. The patient was also provided with a psychiatric referral to assess for the appropriateness of medical intervention.\n\n ## Figures\n\n \n*Page 5 of 6*",
"pagination": {
"current_page": 5,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914556,
"choiceText": "The features of BPD behaviors are ego-dystonic.",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914557,
"choiceText": "The consequences of BPD behaviors do not become distressing to the patient with BPD.",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914558,
"choiceText": "The features of BPD behaviors are ego-syntonic.",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914559,
"choiceText": "The behaviors of mood disorders do not become distressing to the patient.",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 5,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620037,
"questionText": "Which of the following about BPD behaviors is accurate?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "A Distraught Man Engaging in Self-Injury"
},
{
"authors": "Jeffrey S. Forrest, MD; Alexander B. Shortridge",
"content": [],
"date": "February 07, 2025",
"figures": [],
"markdown": "# A Distraught Man Engaging in Self-Injury\n\n **Authors:** Jeffrey S. Forrest, MD; Alexander B. Shortridge \n **Date:** February 07, 2025\n\n ## Content\n\n \n\n ## Figures\n\n \n*Page 6 of 6*",
"pagination": {
"current_page": 6,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1526224,
"choiceText": "Shifts in mood",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526225,
"choiceText": "Impulsivity",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526226,
"choiceText": "Decreased need for sleep",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526227,
"choiceText": "Suicidal behavior",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526228,
"choiceText": "Anger and irritability",
"correct": false,
"displayOrder": 5,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Patients with BPD often experience sleep disturbances, including increased sleep-onset latency, low sleep efficiency, and nightmares. Patients with bipolar disorders often experience a reduced need for sleep during a manic episode and more classically demonstrate excessive sleepiness (hypersomnia) during depressive episodes.",
"displayOrder": 2,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 489045,
"questionText": "Which of the following characteristics is more commonly associated with bipolar disorders as opposed to BPD?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1526229,
"choiceText": "Medications do not effectively treat BPD",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526230,
"choiceText": "Medications may be useful adjunctively but may not maintain their effectiveness",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526231,
"choiceText": "Medications are always useful in the treatment of BPD",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526232,
"choiceText": "Antipsychotic agents should never be prescribed in the treatment of BPD",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "No medication has been approved for the treatment of BPD. However, pharmacologic agents in many classes may be used adjunctively to treat symptoms associated with BPD. Although some patients with BPD may respond well to medication initially, few respond satisfactorily over an extended period,<sup>[18]</sup> and duration of pharmacologic treatment should be time limited.",
"displayOrder": 3,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 489046,
"questionText": "Which of the following statements is most accurate about medication use in treating BPD?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "A Distraught Man Engaging in Self-Injury"
}
] | [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1526219,
"choiceText": "Bipolar disorder",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526220,
"choiceText": "Adjustment disorder",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526221,
"choiceText": "Histrionic personality disorder",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526222,
"choiceText": "Borderline personality disorder",
"correct": true,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526223,
"choiceText": "Posttraumatic stress disorder",
"correct": false,
"displayOrder": 5,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 489044,
"questionText": "Based only on these findings, which of the following is the most likely diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914552,
"choiceText": "Genetic factors are the main factor in the onset of BPD.",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914553,
"choiceText": "Early environmental factors play a role in BPD pathogenesis.",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914554,
"choiceText": "BPD and posttraumatic stress disorder do not occur concomitantly.",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914555,
"choiceText": "BPD primarily affects males.",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 4,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620036,
"questionText": "Which of the following statements about BPD is correct?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914556,
"choiceText": "The features of BPD behaviors are ego-dystonic.",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914557,
"choiceText": "The consequences of BPD behaviors do not become distressing to the patient with BPD.",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914558,
"choiceText": "The features of BPD behaviors are ego-syntonic.",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914559,
"choiceText": "The behaviors of mood disorders do not become distressing to the patient.",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 5,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620037,
"questionText": "Which of the following about BPD behaviors is accurate?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1526224,
"choiceText": "Shifts in mood",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526225,
"choiceText": "Impulsivity",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526226,
"choiceText": "Decreased need for sleep",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526227,
"choiceText": "Suicidal behavior",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526228,
"choiceText": "Anger and irritability",
"correct": false,
"displayOrder": 5,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Patients with BPD often experience sleep disturbances, including increased sleep-onset latency, low sleep efficiency, and nightmares. Patients with bipolar disorders often experience a reduced need for sleep during a manic episode and more classically demonstrate excessive sleepiness (hypersomnia) during depressive episodes.",
"displayOrder": 2,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 489045,
"questionText": "Which of the following characteristics is more commonly associated with bipolar disorders as opposed to BPD?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1526229,
"choiceText": "Medications do not effectively treat BPD",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526230,
"choiceText": "Medications may be useful adjunctively but may not maintain their effectiveness",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526231,
"choiceText": "Medications are always useful in the treatment of BPD",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1526232,
"choiceText": "Antipsychotic agents should never be prescribed in the treatment of BPD",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "No medication has been approved for the treatment of BPD. However, pharmacologic agents in many classes may be used adjunctively to treat symptoms associated with BPD. Although some patients with BPD may respond well to medication initially, few respond satisfactorily over an extended period,<sup>[18]</sup> and duration of pharmacologic treatment should be time limited.",
"displayOrder": 3,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 489046,
"questionText": "Which of the following statements is most accurate about medication use in treating BPD?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
] |
1002186 | /viewarticle/1002186 | [
{
"authors": "Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP",
"content": [
"Editor's Note: The Case Challenge series includes difficult-to-diagnose conditions, some of which are not frequently encountered by most clinicians, but are nonetheless important to accurately recognize. Test your diagnostic and treatment skills using the following patient scenario and corresponding questions. If you have a case that you would like to suggest for a future Case Challenge, please email us at [email protected] with the subject line \"Case Challenge Suggestion.\" We look forward to hearing from you.",
"A 66-year-old male presents to the emergency room with bloating, abdominal discomfort, weight loss of 40 pounds over the past 6 months, non-bloody diarrhea, halitosis, and poor appetite. He also complained of bruising and chest wall pain from a fall about 5 days prior. The patient has a past medical history of low-grade follicular lymphoma of paraaortic lymph nodes undergoing active surveillance, COPD, coronary artery disease, hypertension, hyperlipidemia, cholecystectomy, and ventral hernia repair. He denied rectal bleeding, subjective fevers, or vomiting.",
"His symptoms began approximately 2 years ago after a colonoscopy with hot snare endoscopic mucosal resection (EMR) of an 18 mm flat transverse colon polyp in piecemeal fashion. Five 11 mm standard Endo clips were applied for the purpose of hemostasis and to close the defect. Biopsy revealed tubular adenoma with no dysplasia. Esophagogastroduodenoscopy (EGD) with gastric biopsies showed intestinal metaplasia but negative for malignancy or Helicobacter pylori. Approximately 6 months later, the patient had a repeat colonoscopy which showed residual polypoid tissue at the scar within the transverse colon which was removed with cold snare. This biopsy also revealed tubular adenoma. Following up after both colonoscopies, he developed the symptoms described above. He was empirically treated for suspected small intestine bacterial overgrowth which did not relieve his symptoms. His symptoms worsened and resulted in him presenting to the emergency department."
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# Chronic Abdominal Pain After Colonoscopy\n\n **Authors:** Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP \n **Date:** February 07, 2025\n\n ## Content\n\n Editor's Note: The Case Challenge series includes difficult-to-diagnose conditions, some of which are not frequently encountered by most clinicians, but are nonetheless important to accurately recognize. Test your diagnostic and treatment skills using the following patient scenario and corresponding questions. If you have a case that you would like to suggest for a future Case Challenge, please email us at [email protected] with the subject line \"Case Challenge Suggestion.\" We look forward to hearing from you.\nA 66-year-old male presents to the emergency room with bloating, abdominal discomfort, weight loss of 40 pounds over the past 6 months, non-bloody diarrhea, halitosis, and poor appetite. He also complained of bruising and chest wall pain from a fall about 5 days prior. The patient has a past medical history of low-grade follicular lymphoma of paraaortic lymph nodes undergoing active surveillance, COPD, coronary artery disease, hypertension, hyperlipidemia, cholecystectomy, and ventral hernia repair. He denied rectal bleeding, subjective fevers, or vomiting.\nHis symptoms began approximately 2 years ago after a colonoscopy with hot snare endoscopic mucosal resection (EMR) of an 18 mm flat transverse colon polyp in piecemeal fashion. Five 11 mm standard Endo clips were applied for the purpose of hemostasis and to close the defect. Biopsy revealed tubular adenoma with no dysplasia. Esophagogastroduodenoscopy (EGD) with gastric biopsies showed intestinal metaplasia but negative for malignancy or Helicobacter pylori. Approximately 6 months later, the patient had a repeat colonoscopy which showed residual polypoid tissue at the scar within the transverse colon which was removed with cold snare. This biopsy also revealed tubular adenoma. Following up after both colonoscopies, he developed the symptoms described above. He was empirically treated for suspected small intestine bacterial overgrowth which did not relieve his symptoms. His symptoms worsened and resulted in him presenting to the emergency department.\n\n ## Figures\n\n \n*Page 1 of 6*",
"pagination": {
"current_page": 1,
"total_pages": 6
},
"questionnaire": [],
"title": "Chronic Abdominal Pain After Colonoscopy"
},
{
"authors": "Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP",
"content": [
"Vitals BP 99/59 (BP Location: Left arm, BP Position: Sitting) | Pulse 67| Temp 36.7 °C (98 °F) (Oral) | Resp 16| Ht 182.9 cm| Wt 87.1 kg (192 lb 0.3 oz) | SpO2 100%| BMI 26.04 kg/m2",
"Physical Exam Constitutional: Not in acute distress, ill appearingHENT: Head: Normocephalic and atraumatic. Extraocular Movements: Extraocular movements intact. Pupils are equal, round, and reactive to light. Dentition is poor, halitosis presentCardiovascular: Normal rate and regular rhythmPulmonary: Pulmonary effort is normal. No respiratory distressChest wall: Bruising on left chestAbdominal: Patient is distended. Abdomen is soft, no tenderness, guarding or rebound. No peritoneal signsSkin: Skin is warm and dryNeurological: No focal deficit present. He is alert and oriented",
"Work up BMP and CBC performed at presentation to surgical service showing hypokalemia to 3.1, hyponatremia and hypochloremia, AKI with creatine of 2.6, and BUN of 25. CBC was unremarkable except for mild anemia. Patient prealbumin was 9.2.Hemoglobin: 11.5 g/dL (reference range: 12-16 g/dL)MCV: 8f fL (reference range: 80-100fL)Fecal calprotectin: 40 ug/mg (reference range: 50-200 ug/mg)Diagnostic imaging included CT chest abdomen and pelvis (Figures 1 and 2) and EGD.",
"Figure 1a and 1b. Axial imaging of gastrocolic fistula shown with red arrow (b) sagittal imaging.",
"Figure 2. Red arrow shows fistulous connection while the yellow arrow shows the endo clips used for hemostasis in the first colonoscopy after hot snare biopsies."
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# Chronic Abdominal Pain After Colonoscopy\n\n **Authors:** Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP \n **Date:** February 07, 2025\n\n ## Content\n\n Vitals BP 99/59 (BP Location: Left arm, BP Position: Sitting) | Pulse 67| Temp 36.7 °C (98 °F) (Oral) | Resp 16| Ht 182.9 cm| Wt 87.1 kg (192 lb 0.3 oz) | SpO2 100%| BMI 26.04 kg/m2\nPhysical Exam Constitutional: Not in acute distress, ill appearingHENT: Head: Normocephalic and atraumatic. Extraocular Movements: Extraocular movements intact. Pupils are equal, round, and reactive to light. Dentition is poor, halitosis presentCardiovascular: Normal rate and regular rhythmPulmonary: Pulmonary effort is normal. No respiratory distressChest wall: Bruising on left chestAbdominal: Patient is distended. Abdomen is soft, no tenderness, guarding or rebound. No peritoneal signsSkin: Skin is warm and dryNeurological: No focal deficit present. He is alert and oriented\nWork up BMP and CBC performed at presentation to surgical service showing hypokalemia to 3.1, hyponatremia and hypochloremia, AKI with creatine of 2.6, and BUN of 25. CBC was unremarkable except for mild anemia. Patient prealbumin was 9.2.Hemoglobin: 11.5 g/dL (reference range: 12-16 g/dL)MCV: 8f fL (reference range: 80-100fL)Fecal calprotectin: 40 ug/mg (reference range: 50-200 ug/mg)Diagnostic imaging included CT chest abdomen and pelvis (Figures 1 and 2) and EGD.\nFigure 1a and 1b. Axial imaging of gastrocolic fistula shown with red arrow (b) sagittal imaging.\nFigure 2. Red arrow shows fistulous connection while the yellow arrow shows the endo clips used for hemostasis in the first colonoscopy after hot snare biopsies.\n\n ## Figures\n\n \n*Page 2 of 6*",
"pagination": {
"current_page": 2,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914854,
"choiceText": "Malignancy",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914855,
"choiceText": "Gastrocolic fistula ",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914856,
"choiceText": "Diverticulitis",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914857,
"choiceText": "Inflammatory bowel disease ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620136,
"questionText": "What is the most likely diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Chronic Abdominal Pain After Colonoscopy"
},
{
"authors": "Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP",
"content": [
"A gastrocolic fistula (GCF) is an abnormal connection between the stomach and the colon, which can lead to clinical symptoms such as weight loss, diarrhea, malnutrition, and signs of intestinal obstruction. Although GCFs are typically associated with malignancy, inflammatory conditions, or trauma, they may also develop as a rare complication after colon procedures, including polypectomies. This case report describes the spontaneous development of a GCF in a patient possibly due to a hot snare EMR of a transverse colon polyp. This likely occurred due to deep tissue injury from cautery which led to a delayed perforation extending through the colon wall and forming a connection into the stomach.",
"Epidemiology of Gastrocolic Fistulas",
"GCFs are an uncommon but clinically significant condition. Their incidence is difficult to quantify due to the rarity of the disorder and the various etiologies that contribute to its development. Traditionally, GCFs are most often associated with malignancies, particularly colonic cancers or gastric cancers that invade adjacent structures. In such cases, the fistula is often the result of direct tumor extension. Other common causes include diverticulitis, inflammatory bowel diseases (IBDs; such as Crohn's disease), gastric peptic ulcer disease, iatrogenic, and trauma (post-surgical or post-injury).",
"While Iatrogenic causes of GCFs are rare, they have been documented in the literature. These cases are typically associated with surgical procedures involving the stomach or colon, such as colorectal resections. This case highlights the possibility of a GCF that occurred after a hot snare EMR of a < 20 mm transverse colon polyp, diagnosed over a year after colonoscopy. GCF due to hot snare EMR/polypectomy has not yet been described in the literature.",
"Clinical Presentation",
"The clinical presentation of a GCF is varied, and patients may exhibit atypical or nonspecific symptoms. The most common symptoms associated with GCFs include:",
"Chronic diarrhea: The presence of fecal material in the stomach or the inability to fully digest food in the stomach can lead to diarrhea due to undigested material being passed into the small and large intestines.",
"Weight loss and malnutrition: The abnormal communication between the stomach and the colon results in inefficient digestion and nutrient absorption, leading to progressive weight loss and electrolyte deficiencies.",
"Abdominal pain: Although this is not always present, it can occur if the fistula causes irritation of the stomach lining or colonic mucosa.",
"Feculent vomiting: In rare cases, the fistula can lead to regurgitation of fecal material, particularly if a portion of the colon becomes distended or obstructed.",
"In this case, the patient was initially presenting with symptoms of intermittent abdominal pain, nausea, extreme halitosis, malnutrition, weight loss, and diarrhea, which gradually worsened over a period of several months. There was no history of fever, gross rectal bleeding, feculent vomiting, or signs of acute obstruction, which made the diagnosis more challenging. The absence of these typical red flags pointed clinicians towards a less acute diagnosis."
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# Chronic Abdominal Pain After Colonoscopy\n\n **Authors:** Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP \n **Date:** February 07, 2025\n\n ## Content\n\n A gastrocolic fistula (GCF) is an abnormal connection between the stomach and the colon, which can lead to clinical symptoms such as weight loss, diarrhea, malnutrition, and signs of intestinal obstruction. Although GCFs are typically associated with malignancy, inflammatory conditions, or trauma, they may also develop as a rare complication after colon procedures, including polypectomies. This case report describes the spontaneous development of a GCF in a patient possibly due to a hot snare EMR of a transverse colon polyp. This likely occurred due to deep tissue injury from cautery which led to a delayed perforation extending through the colon wall and forming a connection into the stomach.\nEpidemiology of Gastrocolic Fistulas\nGCFs are an uncommon but clinically significant condition. Their incidence is difficult to quantify due to the rarity of the disorder and the various etiologies that contribute to its development. Traditionally, GCFs are most often associated with malignancies, particularly colonic cancers or gastric cancers that invade adjacent structures. In such cases, the fistula is often the result of direct tumor extension. Other common causes include diverticulitis, inflammatory bowel diseases (IBDs; such as Crohn's disease), gastric peptic ulcer disease, iatrogenic, and trauma (post-surgical or post-injury).\nWhile Iatrogenic causes of GCFs are rare, they have been documented in the literature. These cases are typically associated with surgical procedures involving the stomach or colon, such as colorectal resections. This case highlights the possibility of a GCF that occurred after a hot snare EMR of a < 20 mm transverse colon polyp, diagnosed over a year after colonoscopy. GCF due to hot snare EMR/polypectomy has not yet been described in the literature.\nClinical Presentation\nThe clinical presentation of a GCF is varied, and patients may exhibit atypical or nonspecific symptoms. The most common symptoms associated with GCFs include:\nChronic diarrhea: The presence of fecal material in the stomach or the inability to fully digest food in the stomach can lead to diarrhea due to undigested material being passed into the small and large intestines.\nWeight loss and malnutrition: The abnormal communication between the stomach and the colon results in inefficient digestion and nutrient absorption, leading to progressive weight loss and electrolyte deficiencies.\nAbdominal pain: Although this is not always present, it can occur if the fistula causes irritation of the stomach lining or colonic mucosa.\nFeculent vomiting: In rare cases, the fistula can lead to regurgitation of fecal material, particularly if a portion of the colon becomes distended or obstructed.\nIn this case, the patient was initially presenting with symptoms of intermittent abdominal pain, nausea, extreme halitosis, malnutrition, weight loss, and diarrhea, which gradually worsened over a period of several months. There was no history of fever, gross rectal bleeding, feculent vomiting, or signs of acute obstruction, which made the diagnosis more challenging. The absence of these typical red flags pointed clinicians towards a less acute diagnosis.\n\n ## Figures\n\n \n*Page 3 of 6*",
"pagination": {
"current_page": 3,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914854,
"choiceText": "Malignancy",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914855,
"choiceText": "Gastrocolic fistula ",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914856,
"choiceText": "Diverticulitis",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914857,
"choiceText": "Inflammatory bowel disease ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620136,
"questionText": "What is the most likely diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Chronic Abdominal Pain After Colonoscopy"
},
{
"authors": "Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP",
"content": [
"Differential Diagnosis",
"The differential diagnosis for a GCF in a post-polypectomy patient includes several conditions, which must be ruled out to establish an accurate diagnosis:",
"Post-surgical adhesions: Adhesions after colorectal surgery can lead to bowel obstruction, but they do not generally cause a direct fistulous connection between the stomach and the colon.",
"Colonic or gastric malignancy: This must be considered given that malignancies are the most common cause of GCF. However, the absence of a history of malignancy, normal oncological work-up, and histopathological examination of the polypectomy specimen ruled out cancer. Pathologies of EGD and colonoscopy prior to symptoms were all negative for malignancy in this patient.",
"History of lymphoma: Given the history of lymphoma in this patient, this could have been causing symptoms. Lymphomas have been known to cause gastric outlet syndrome from compressive pathologies; however, this patient had low grade lymphoma of the paraaortic lymph nodes, did not receive treatment, and had no disease progression during surveillance.",
"IBD: Conditions like Crohn's disease can result in fistulas between the colon and other abdominal organs, including the stomach. However, the absence of systemic IBD symptoms, such as bloody diarrhea or a history of chronic IBD, made this diagnosis less likely.",
"Diverticulitis: While diverticulitis can sometimes result in fistula formation, the patient did not have a history or symptoms suggestive of diverticular disease.",
"Peptic ulcer disease: Although peptic ulcers can cause a gastroduodenal fistula, the lack of ulcer-related symptoms and normal gastric imaging studies made this unlikely.",
"Diagnosis",
"The diagnosis of a GCF requires a high index of suspicion—particularly in patients who underwent colon surgery—normally involving transverse colon or gastric surgery. Initial clinical evaluation typically includes a thorough history and physical, radiologic imaging and endoscopy.",
"History and Physical Examination: A thorough clinical history will reveal chronicity of the patient's symptoms. Constitutional symptoms may help ascertain the etiology if oncological disease is suspected. Upper GI symptoms such as vomiting or feculent vomiting are specific signs. History may also reveal a temporal relationship between the surgical procedure and the onset of symptoms. Physical examination may reveal a distended abdomen with upper abdominal tenderness. Cachectic or pale appearance may point towards cancer or anemia.",
"Imaging Studies: Imaging studies play a key role in confirming the diagnosis of a GCF. Contrast-enhanced CT of the abdomen with oral contrast is often the first-line imaging modality and can help identify abnormal communication between the stomach and colon. Barium upper GI radiography may also display contrast filling of colon from the stomach.",
"Endoscopy: Flexible sigmoidoscopy or colonoscopy may be used to directly visualize the colon and assess any evidence of a fistula or inflammatory changes. Upper gastrointestinal endoscopy can also help visualize any gastric lesions or confirm the presence of a fistula opening within the stomach. Transition from classical stomach rugal folds to circular colonic mucosa would be evident.",
"Figure 3. Upper endoscopy of gastrocolic fistula (a) normal esophagus (b) pylorus (c/d) fistulous connection with colonic mucosa seen (e) transverse colon with stool that was irrigated",
"In this patient, the combination of clinical suspicion, CT imaging, and upper gastrointestinal endoscopy led to the diagnosis of a GCF. The patient did not have any signs of malignancy, and histopathology of the excised colon polyp was benign."
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# Chronic Abdominal Pain After Colonoscopy\n\n **Authors:** Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP \n **Date:** February 07, 2025\n\n ## Content\n\n Differential Diagnosis\nThe differential diagnosis for a GCF in a post-polypectomy patient includes several conditions, which must be ruled out to establish an accurate diagnosis:\nPost-surgical adhesions: Adhesions after colorectal surgery can lead to bowel obstruction, but they do not generally cause a direct fistulous connection between the stomach and the colon.\nColonic or gastric malignancy: This must be considered given that malignancies are the most common cause of GCF. However, the absence of a history of malignancy, normal oncological work-up, and histopathological examination of the polypectomy specimen ruled out cancer. Pathologies of EGD and colonoscopy prior to symptoms were all negative for malignancy in this patient.\nHistory of lymphoma: Given the history of lymphoma in this patient, this could have been causing symptoms. Lymphomas have been known to cause gastric outlet syndrome from compressive pathologies; however, this patient had low grade lymphoma of the paraaortic lymph nodes, did not receive treatment, and had no disease progression during surveillance.\nIBD: Conditions like Crohn's disease can result in fistulas between the colon and other abdominal organs, including the stomach. However, the absence of systemic IBD symptoms, such as bloody diarrhea or a history of chronic IBD, made this diagnosis less likely.\nDiverticulitis: While diverticulitis can sometimes result in fistula formation, the patient did not have a history or symptoms suggestive of diverticular disease.\nPeptic ulcer disease: Although peptic ulcers can cause a gastroduodenal fistula, the lack of ulcer-related symptoms and normal gastric imaging studies made this unlikely.\nDiagnosis\nThe diagnosis of a GCF requires a high index of suspicion—particularly in patients who underwent colon surgery—normally involving transverse colon or gastric surgery. Initial clinical evaluation typically includes a thorough history and physical, radiologic imaging and endoscopy.\nHistory and Physical Examination: A thorough clinical history will reveal chronicity of the patient's symptoms. Constitutional symptoms may help ascertain the etiology if oncological disease is suspected. Upper GI symptoms such as vomiting or feculent vomiting are specific signs. History may also reveal a temporal relationship between the surgical procedure and the onset of symptoms. Physical examination may reveal a distended abdomen with upper abdominal tenderness. Cachectic or pale appearance may point towards cancer or anemia.\nImaging Studies: Imaging studies play a key role in confirming the diagnosis of a GCF. Contrast-enhanced CT of the abdomen with oral contrast is often the first-line imaging modality and can help identify abnormal communication between the stomach and colon. Barium upper GI radiography may also display contrast filling of colon from the stomach.\nEndoscopy: Flexible sigmoidoscopy or colonoscopy may be used to directly visualize the colon and assess any evidence of a fistula or inflammatory changes. Upper gastrointestinal endoscopy can also help visualize any gastric lesions or confirm the presence of a fistula opening within the stomach. Transition from classical stomach rugal folds to circular colonic mucosa would be evident.\nFigure 3. Upper endoscopy of gastrocolic fistula (a) normal esophagus (b) pylorus (c/d) fistulous connection with colonic mucosa seen (e) transverse colon with stool that was irrigated\nIn this patient, the combination of clinical suspicion, CT imaging, and upper gastrointestinal endoscopy led to the diagnosis of a GCF. The patient did not have any signs of malignancy, and histopathology of the excised colon polyp was benign.\n\n ## Figures\n\n \n*Page 4 of 6*",
"pagination": {
"current_page": 4,
"total_pages": 6
},
"questionnaire": [],
"title": "Chronic Abdominal Pain After Colonoscopy"
},
{
"authors": "Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP",
"content": [
"Treatment and Management",
"The management of a GCF depends on its size, etiology, and the patient’s overall clinical condition. In this case, the fistula was identified early, and the patient was initially managed conservatively with nutritional support and close monitoring.",
"Conservative Management: Small fistulas may be treated conservatively with bowel rest, nutritional support, and antisecretory medications such as proton pump inhibitors to reduce gastric acid production and promote healing.",
"Endoscopic Interventions: Endoscopic closure of the fistula using clips or suturing devices is an option for small, accessible fistulas, though this approach is not always successful in larger or more complex fistulas.",
"Surgical Intervention: For larger or symptomatic fistulas that do not respond to conservative or endoscopic management, surgical resection may be required.",
"In this patient, a surgical approach was used to repair the fistulous tract given the size and the complexity of the lesion. We resected the segment of transverse colon and the portion of the stomach along the greater curvature with colocolonic anastomosis and repair of the gastrotomy.",
"Clinical Course",
"Following the surgical repair, the patient had resolution of the initial symptoms of abdominal pain, diarrhea, and dietary intolerance. Unfortunately, the patient developed atrial flutter post-operatively. The arrhythmia resolved and the patient was discharged on a regular diet on post-op day 9 with plans for follow-up to monitor for any recurrence of symptoms or complications.",
"Over the next months, the patient remained asymptomatic with normal gastrointestinal function. A follow up CT scan revealed restored anatomy. He was seen in clinic, and original symptoms have been resolved. He now suffers from some constipation relieved with laxatives.",
"Conclusion",
"Polyp removal during colonoscopy has resulted in a significant reduction in mortality rates associated with colorectal cancer. Various methods can be used for safe removal of polyps endoscopically. Gastroenterologists can not only cold snare polyps but perform full thickness resections of large polyps using EMR and or endoscopic submucosal resection techniques that otherwise require surgical resection. Current evidence supports the use of cold snare EMR over hot EMR given its decreased delayed bleeding and risk of full thickness injury even for polyps larger than 20 mm.",
"GCFs are a rare but serious complication of hot snare polypectomies. Clinicians should consider GCF in the differential diagnosis for patients presenting with persistent gastrointestinal symptoms, especially when there is no clear etiology. Early diagnosis with imaging and endoscopy, followed by appropriate management, typically leads to favorable outcomes. This case underscores the importance of recognizing this rare complication and highlights the potential for spontaneous development of GCF following relatively routine colon procedures."
],
"date": "February 07, 2025",
"figures": [],
"markdown": "# Chronic Abdominal Pain After Colonoscopy\n\n **Authors:** Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP \n **Date:** February 07, 2025\n\n ## Content\n\n Treatment and Management\nThe management of a GCF depends on its size, etiology, and the patient’s overall clinical condition. In this case, the fistula was identified early, and the patient was initially managed conservatively with nutritional support and close monitoring.\nConservative Management: Small fistulas may be treated conservatively with bowel rest, nutritional support, and antisecretory medications such as proton pump inhibitors to reduce gastric acid production and promote healing.\nEndoscopic Interventions: Endoscopic closure of the fistula using clips or suturing devices is an option for small, accessible fistulas, though this approach is not always successful in larger or more complex fistulas.\nSurgical Intervention: For larger or symptomatic fistulas that do not respond to conservative or endoscopic management, surgical resection may be required.\nIn this patient, a surgical approach was used to repair the fistulous tract given the size and the complexity of the lesion. We resected the segment of transverse colon and the portion of the stomach along the greater curvature with colocolonic anastomosis and repair of the gastrotomy.\nClinical Course\nFollowing the surgical repair, the patient had resolution of the initial symptoms of abdominal pain, diarrhea, and dietary intolerance. Unfortunately, the patient developed atrial flutter post-operatively. The arrhythmia resolved and the patient was discharged on a regular diet on post-op day 9 with plans for follow-up to monitor for any recurrence of symptoms or complications.\nOver the next months, the patient remained asymptomatic with normal gastrointestinal function. A follow up CT scan revealed restored anatomy. He was seen in clinic, and original symptoms have been resolved. He now suffers from some constipation relieved with laxatives.\nConclusion\nPolyp removal during colonoscopy has resulted in a significant reduction in mortality rates associated with colorectal cancer. Various methods can be used for safe removal of polyps endoscopically. Gastroenterologists can not only cold snare polyps but perform full thickness resections of large polyps using EMR and or endoscopic submucosal resection techniques that otherwise require surgical resection. Current evidence supports the use of cold snare EMR over hot EMR given its decreased delayed bleeding and risk of full thickness injury even for polyps larger than 20 mm.\nGCFs are a rare but serious complication of hot snare polypectomies. Clinicians should consider GCF in the differential diagnosis for patients presenting with persistent gastrointestinal symptoms, especially when there is no clear etiology. Early diagnosis with imaging and endoscopy, followed by appropriate management, typically leads to favorable outcomes. This case underscores the importance of recognizing this rare complication and highlights the potential for spontaneous development of GCF following relatively routine colon procedures.\n\n ## Figures\n\n \n*Page 5 of 6*",
"pagination": {
"current_page": 5,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914858,
"choiceText": "Iatrogenic injury during colon procedures ",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914859,
"choiceText": "Malignancies such as gastric or colonic cancers ",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914860,
"choiceText": "IBD ",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914861,
"choiceText": "Diverticulitis ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "GCFs are most commonly associated with malignancies, particularly gastric or colonic cancers. These cancers can invade adjacent structures, leading to fistula formation. While other etiologies such as IBD, diverticulitis, and iatrogenic injury are possible causes, malignancies remain the predominant underlying condition in most cases. ",
"displayOrder": 2,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620137,
"questionText": "What is the most common underlying cause of GCFs? ",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914862,
"choiceText": "Endoscopy",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914863,
"choiceText": "Colonoscopy alone ",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914864,
"choiceText": "Contrast-enhanced CT with oral contrast ",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914865,
"choiceText": "Plain abdominal x-ray ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Contrast-enhanced CT with oral contrast is the first-line imaging modality for diagnosing a GCF. It allows visualization of abnormal communication between the stomach and colon and provides detailed anatomical information. While endoscopic techniques (eg, colonoscopy and upper GI endoscopy) are valuable for direct visualization and further characterization, they are typically adjunctive to CT imaging. Plain x-rays and ultrasound lack the sensitivity and specificity to reliably identify GCFs. ",
"displayOrder": 3,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620138,
"questionText": "Which diagnostic modality is most commonly used to confirm the presence of a GCF? ",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Chronic Abdominal Pain After Colonoscopy"
},
{
"authors": "Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP",
"content": [],
"date": "February 07, 2025",
"figures": [],
"markdown": "# Chronic Abdominal Pain After Colonoscopy\n\n **Authors:** Assar Rather, MD; Lynnsey M. Rebner, DO; Hamdan Mallick, MD; Amber Jacobson, DO; Adrianne Fisher, FNP \n **Date:** February 07, 2025\n\n ## Content\n\n \n\n ## Figures\n\n \n*Page 6 of 6*",
"pagination": {
"current_page": 6,
"total_pages": 6
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914858,
"choiceText": "Iatrogenic injury during colon procedures ",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914859,
"choiceText": "Malignancies such as gastric or colonic cancers ",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914860,
"choiceText": "IBD ",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914861,
"choiceText": "Diverticulitis ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "GCFs are most commonly associated with malignancies, particularly gastric or colonic cancers. These cancers can invade adjacent structures, leading to fistula formation. While other etiologies such as IBD, diverticulitis, and iatrogenic injury are possible causes, malignancies remain the predominant underlying condition in most cases. ",
"displayOrder": 2,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620137,
"questionText": "What is the most common underlying cause of GCFs? ",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914862,
"choiceText": "Endoscopy",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914863,
"choiceText": "Colonoscopy alone ",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914864,
"choiceText": "Contrast-enhanced CT with oral contrast ",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914865,
"choiceText": "Plain abdominal x-ray ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Contrast-enhanced CT with oral contrast is the first-line imaging modality for diagnosing a GCF. It allows visualization of abnormal communication between the stomach and colon and provides detailed anatomical information. While endoscopic techniques (eg, colonoscopy and upper GI endoscopy) are valuable for direct visualization and further characterization, they are typically adjunctive to CT imaging. Plain x-rays and ultrasound lack the sensitivity and specificity to reliably identify GCFs. ",
"displayOrder": 3,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620138,
"questionText": "Which diagnostic modality is most commonly used to confirm the presence of a GCF? ",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Chronic Abdominal Pain After Colonoscopy"
}
] | [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914854,
"choiceText": "Malignancy",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914855,
"choiceText": "Gastrocolic fistula ",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914856,
"choiceText": "Diverticulitis",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914857,
"choiceText": "Inflammatory bowel disease ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620136,
"questionText": "What is the most likely diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914858,
"choiceText": "Iatrogenic injury during colon procedures ",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914859,
"choiceText": "Malignancies such as gastric or colonic cancers ",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914860,
"choiceText": "IBD ",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914861,
"choiceText": "Diverticulitis ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "GCFs are most commonly associated with malignancies, particularly gastric or colonic cancers. These cancers can invade adjacent structures, leading to fistula formation. While other etiologies such as IBD, diverticulitis, and iatrogenic injury are possible causes, malignancies remain the predominant underlying condition in most cases. ",
"displayOrder": 2,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620137,
"questionText": "What is the most common underlying cause of GCFs? ",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914862,
"choiceText": "Endoscopy",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914863,
"choiceText": "Colonoscopy alone ",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914864,
"choiceText": "Contrast-enhanced CT with oral contrast ",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914865,
"choiceText": "Plain abdominal x-ray ",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Contrast-enhanced CT with oral contrast is the first-line imaging modality for diagnosing a GCF. It allows visualization of abnormal communication between the stomach and colon and provides detailed anatomical information. While endoscopic techniques (eg, colonoscopy and upper GI endoscopy) are valuable for direct visualization and further characterization, they are typically adjunctive to CT imaging. Plain x-rays and ultrasound lack the sensitivity and specificity to reliably identify GCFs. ",
"displayOrder": 3,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 620138,
"questionText": "Which diagnostic modality is most commonly used to confirm the presence of a GCF? ",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
] |
834367 | /viewarticle/834367 | [
{
"authors": "Robert S. Bader, MD",
"content": [
"Editor's Note:\nThe Case Challenge series includes difficult-to-diagnose conditions, some of which are not frequently encountered by most clinicians, but are nonetheless important to accurately recognize. Test your diagnostic and treatment skills using the following patient scenario and corresponding questions. If you have a case that you would like to suggest for a future Case Challenge, please email us at [email protected] with the subject line \"Case Challenge Suggestion.\" We look forward to hearing from you.",
"A 51-year-old White man presents to the dermatologist for removal of an epidermal cyst on his left lower eyelid. He has no other complaints. During discussion about the treatment of his cyst, two lesions are seen on the right arm. He was unaware of these lesions; no history could be provided.",
"The patient's medical history is unremarkable, except for a right inguinal hernia repair. He takes no medications, has no allergies, consumes one alcoholic drink daily, and smokes cigarettes on occasion. He has worked inside his entire life and grew up in South Florida. He reports having several blistering sunburns as a child. There is no family history of skin cancer. Review of the patient's symptoms is unremarkable.",
"Two solitary, fairly well-circumscribed, 8-mm, pink macules with scale were found on the patient's right arm (Figure 1).",
"Figure 1.",
"With compression, the lesions blanch slightly but not completely. This prompts a complete skin examination, which is performed and is otherwise unremarkable, with the exception of a 4-mm cyst on the left lower eyelid. Biopsy specimens are obtained from both lesions on his arm using the shave technique, and they are sent for pathologic evaluation."
],
"date": "February 04, 2025",
"figures": [
{
"caption": "Figure 1.",
"image_url": "https://img.medscapestatic.com/article/834/367/834367-thumb-1.jpg"
}
],
"markdown": "# Lesions on a 51-Year-Old Man With Eyelid Cyst\n\n **Authors:** Robert S. Bader, MD \n **Date:** February 04, 2025\n\n ## Content\n\n Editor's Note:\nThe Case Challenge series includes difficult-to-diagnose conditions, some of which are not frequently encountered by most clinicians, but are nonetheless important to accurately recognize. Test your diagnostic and treatment skills using the following patient scenario and corresponding questions. If you have a case that you would like to suggest for a future Case Challenge, please email us at [email protected] with the subject line \"Case Challenge Suggestion.\" We look forward to hearing from you.\nA 51-year-old White man presents to the dermatologist for removal of an epidermal cyst on his left lower eyelid. He has no other complaints. During discussion about the treatment of his cyst, two lesions are seen on the right arm. He was unaware of these lesions; no history could be provided.\nThe patient's medical history is unremarkable, except for a right inguinal hernia repair. He takes no medications, has no allergies, consumes one alcoholic drink daily, and smokes cigarettes on occasion. He has worked inside his entire life and grew up in South Florida. He reports having several blistering sunburns as a child. There is no family history of skin cancer. Review of the patient's symptoms is unremarkable.\nTwo solitary, fairly well-circumscribed, 8-mm, pink macules with scale were found on the patient's right arm (Figure 1).\nFigure 1.\nWith compression, the lesions blanch slightly but not completely. This prompts a complete skin examination, which is performed and is otherwise unremarkable, with the exception of a 4-mm cyst on the left lower eyelid. Biopsy specimens are obtained from both lesions on his arm using the shave technique, and they are sent for pathologic evaluation.\n\n ## Figures\n\n **Figure 1.** \n \n\n\n*Page 1 of 5*",
"pagination": {
"current_page": 1,
"total_pages": 5
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 785871,
"choiceText": "Nummular dermatitis",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785873,
"choiceText": "Pityriasis rosea",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785875,
"choiceText": "Superficial basal cell carcinoma",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785877,
"choiceText": "Guttate psoriasis",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 246237,
"questionText": "On the basis of the history, physical examination, and workup, what is the diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Lesions on a 51-Year-Old Man With Eyelid Cyst"
},
{
"authors": "Robert S. Bader, MD",
"content": [
"Basal cell carcinoma is the most common form of skin cancer in the United States, Australia, and many other countries with a large White population. Persons of color can develop basal cell carcinoma, especially lighter-skinned individuals with a history of repeated, prolonged, recreational or occupational sun exposure.[1]",
"Risk factors include fair complexion, red hair, blue eyes, history of intermittent intense sun exposure, history of blistering sunburns as a child, radiation therapy, family history of basal cell carcinoma, and immunosuppression.[2] Once an individual has had a basal cell carcinoma, the risk of developing a subsequent basal cell carcinoma is about 50% within 5 years.[3]",
"Basal cell carcinoma presents with several different clinical morphologies, which can widely vary.[4] The clinician must be aware of these different clinical presentations. In addition, these clinical types may have different histologic features, which greatly influence the form of therapy that one would choose (see Figure 2).",
"Figure 2.",
"The most common type of basal cell carcinoma is nodular. It usually presents as a round, pearly, or flesh-colored papule with telangiectasia. Central ulceration is common, especially with larger tumors. Bleeding with the slightest trauma is common. These tumors are found most commonly on the face, head, and neck, especially the nose.[5] The forehead, ears (especially in men), cheeks, and periocular skin are commonly affected, although any part of the body may be involved.",
"Micronodular tumors do not have a classic appearance; the growth pattern of small collections of tumor cells make treatment with curettage less successful. Cystic basal cell carcinomas present as a blue-gray, dome-shaped, cystic papule or nodule. Clinically, they often resemble eccrine or apocrine hidrocystomas. Pigmented variants comprise 6% of all basal cell carcinomas. They have all of the features of a nodular basal cell carcinoma, but with brown or black pigment in some or most areas of the tumor. Treatment with ionizing radiation does not resolve the pigmentation at the site of the tumor.",
"Superficial basal cell carcinoma is an extremely common type that is also termed superficial multicentric basal cell carcinoma. This type accounts for about 15% of all basal cell carcinomas. They are seen mostly on the upper trunk (45%), shoulders, or distal extremities (15%), appearing as an erythematous, well-circumscribed macule, patch, or plaque, often with fine scale.[5] Close examination may show telangiectasia or a pearly translucence, especially at the border. Occasionally, the tumors heal in one area, leaving a white, slightly atrophic scar as the tumor spreads to neighboring skin. The lesions enlarge slowly and are easily misdiagnosed as psoriasis or eczema. This tumor is the most common type seen in patients with HIV infection.",
"The infiltrative subtype is aggressive and is characterized microscopically by tumor cells infiltrating into the dermis as strands between the collagen fibers. It does not have the scarlike appearance of the morpheaform type of basal cell carcinoma. This type of growth pattern makes them less amenable to curettage.",
"The morpheaform, sclerotic, or cicatricial variant accounts for less than 6% of all basal cell carcinomas and often presents as a yellow-waxy or white scarlike patch or plaque that rarely ulcerates, with 95% presenting on the head or neck. These tumors are usually flat or slightly depressed, fibrotic, and firm, lacking the typical findings of a superficial or nodular basal cell carcinoma. Histologically, tumor cells grow as strands amid a densely packed hypocellular connective tissue."
],
"date": "February 04, 2025",
"figures": [
{
"caption": "Figure 2.",
"image_url": "https://img.medscapestatic.com/article/834/367/834367-thumb-2.jpg"
}
],
"markdown": "# Lesions on a 51-Year-Old Man With Eyelid Cyst\n\n **Authors:** Robert S. Bader, MD \n **Date:** February 04, 2025\n\n ## Content\n\n Basal cell carcinoma is the most common form of skin cancer in the United States, Australia, and many other countries with a large White population. Persons of color can develop basal cell carcinoma, especially lighter-skinned individuals with a history of repeated, prolonged, recreational or occupational sun exposure.[1]\nRisk factors include fair complexion, red hair, blue eyes, history of intermittent intense sun exposure, history of blistering sunburns as a child, radiation therapy, family history of basal cell carcinoma, and immunosuppression.[2] Once an individual has had a basal cell carcinoma, the risk of developing a subsequent basal cell carcinoma is about 50% within 5 years.[3]\nBasal cell carcinoma presents with several different clinical morphologies, which can widely vary.[4] The clinician must be aware of these different clinical presentations. In addition, these clinical types may have different histologic features, which greatly influence the form of therapy that one would choose (see Figure 2).\nFigure 2.\nThe most common type of basal cell carcinoma is nodular. It usually presents as a round, pearly, or flesh-colored papule with telangiectasia. Central ulceration is common, especially with larger tumors. Bleeding with the slightest trauma is common. These tumors are found most commonly on the face, head, and neck, especially the nose.[5] The forehead, ears (especially in men), cheeks, and periocular skin are commonly affected, although any part of the body may be involved.\nMicronodular tumors do not have a classic appearance; the growth pattern of small collections of tumor cells make treatment with curettage less successful. Cystic basal cell carcinomas present as a blue-gray, dome-shaped, cystic papule or nodule. Clinically, they often resemble eccrine or apocrine hidrocystomas. Pigmented variants comprise 6% of all basal cell carcinomas. They have all of the features of a nodular basal cell carcinoma, but with brown or black pigment in some or most areas of the tumor. Treatment with ionizing radiation does not resolve the pigmentation at the site of the tumor.\nSuperficial basal cell carcinoma is an extremely common type that is also termed superficial multicentric basal cell carcinoma. This type accounts for about 15% of all basal cell carcinomas. They are seen mostly on the upper trunk (45%), shoulders, or distal extremities (15%), appearing as an erythematous, well-circumscribed macule, patch, or plaque, often with fine scale.[5] Close examination may show telangiectasia or a pearly translucence, especially at the border. Occasionally, the tumors heal in one area, leaving a white, slightly atrophic scar as the tumor spreads to neighboring skin. The lesions enlarge slowly and are easily misdiagnosed as psoriasis or eczema. This tumor is the most common type seen in patients with HIV infection.\nThe infiltrative subtype is aggressive and is characterized microscopically by tumor cells infiltrating into the dermis as strands between the collagen fibers. It does not have the scarlike appearance of the morpheaform type of basal cell carcinoma. This type of growth pattern makes them less amenable to curettage.\nThe morpheaform, sclerotic, or cicatricial variant accounts for less than 6% of all basal cell carcinomas and often presents as a yellow-waxy or white scarlike patch or plaque that rarely ulcerates, with 95% presenting on the head or neck. These tumors are usually flat or slightly depressed, fibrotic, and firm, lacking the typical findings of a superficial or nodular basal cell carcinoma. Histologically, tumor cells grow as strands amid a densely packed hypocellular connective tissue.\n\n ## Figures\n\n **Figure 2.** \n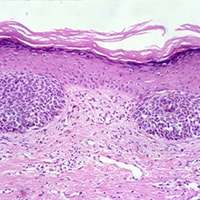 \n\n\n*Page 2 of 5*",
"pagination": {
"current_page": 2,
"total_pages": 5
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 785871,
"choiceText": "Nummular dermatitis",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785873,
"choiceText": "Pityriasis rosea",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785875,
"choiceText": "Superficial basal cell carcinoma",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785877,
"choiceText": "Guttate psoriasis",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 246237,
"questionText": "On the basis of the history, physical examination, and workup, what is the diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Lesions on a 51-Year-Old Man With Eyelid Cyst"
},
{
"authors": "Robert S. Bader, MD",
"content": [
"Of the subtypes listed, the most common types of basal cell carcinoma, ranked in order, are (1) nodular, (2) superficial (spreading), (3) infiltrative, and (4) morpheaform (sclerosing).",
"When a basal cell carcinoma is neglected, a large ulceration may form. A pearly border may or may not be present. This rodent ulcer variant is easily misdiagnosed as a venous stasis ulcer when on the lower extremity. Solitary basal cell carcinomas in young persons are typically located in the region of embryonic clefts on the face. Because they are often deeply invasive, complete surgical removal is recommended; this technique is superior to curettage. Teenagers and children can be affected, and the condition may be associated with basal cell nevus syndrome or nevus sebaceus.",
"Basal cell carcinoma is typically a slow-growing tumor that may ulcerate as it enlarges. Typically, tumors tend to bleed with the slightest trauma and are not painful. Some lesions heal spontaneously and can reulcerate or heal with scar.",
"Metastasis is extremely rare, occurring in less than 0.55% of cases. The tumor requires its supporting stroma for survival, making metastasis rare. Metastasis is twice as common in men as in women, and immunosuppression is not a risk factor. Most basal cell carcinomas that do metastasize are on the head and neck, are large, and are recurrent. Perineural or intravascular basal cell carcinoma are risk factors for metastasis. The regional lymph nodes are the most common site of metastasis, followed by lung, bone, skin, liver, and pleura. Tumors have been reported to metastasize 45 years after the primary diagnosis. Once metastasis occurs, less than 20% of patients survive 1 year.",
"A definitive diagnosis can usually be made easily with a skin biopsy, which should be performed in all cases to determine the histologic subtype of tumor. In nearly all cases, a shave biopsy is all that is required. In the case of pigmented basal cell carcinoma, which can have some clinical features of a malignant melanoma, a punch biopsy is recommended because if the lesion proves to be a melanoma, recording the depth of the tumor is essential.",
"In addition, if a basal cell carcinoma is clinically suspected, but not found with a shave biopsy, a punch biopsy may be helpful in establishing a diagnosis, especially when infiltrative and morpheaform types of basal cell carcinoma are suspected. Because these tumors rarely metastasize, additional laboratory and imaging studies are not commonly indicated unless involvement of deeper structures, such as bone, is clinically suspected, in which case CT or radiography can be used."
],
"date": "February 04, 2025",
"figures": [],
"markdown": "# Lesions on a 51-Year-Old Man With Eyelid Cyst\n\n **Authors:** Robert S. Bader, MD \n **Date:** February 04, 2025\n\n ## Content\n\n Of the subtypes listed, the most common types of basal cell carcinoma, ranked in order, are (1) nodular, (2) superficial (spreading), (3) infiltrative, and (4) morpheaform (sclerosing).\nWhen a basal cell carcinoma is neglected, a large ulceration may form. A pearly border may or may not be present. This rodent ulcer variant is easily misdiagnosed as a venous stasis ulcer when on the lower extremity. Solitary basal cell carcinomas in young persons are typically located in the region of embryonic clefts on the face. Because they are often deeply invasive, complete surgical removal is recommended; this technique is superior to curettage. Teenagers and children can be affected, and the condition may be associated with basal cell nevus syndrome or nevus sebaceus.\nBasal cell carcinoma is typically a slow-growing tumor that may ulcerate as it enlarges. Typically, tumors tend to bleed with the slightest trauma and are not painful. Some lesions heal spontaneously and can reulcerate or heal with scar.\nMetastasis is extremely rare, occurring in less than 0.55% of cases. The tumor requires its supporting stroma for survival, making metastasis rare. Metastasis is twice as common in men as in women, and immunosuppression is not a risk factor. Most basal cell carcinomas that do metastasize are on the head and neck, are large, and are recurrent. Perineural or intravascular basal cell carcinoma are risk factors for metastasis. The regional lymph nodes are the most common site of metastasis, followed by lung, bone, skin, liver, and pleura. Tumors have been reported to metastasize 45 years after the primary diagnosis. Once metastasis occurs, less than 20% of patients survive 1 year.\nA definitive diagnosis can usually be made easily with a skin biopsy, which should be performed in all cases to determine the histologic subtype of tumor. In nearly all cases, a shave biopsy is all that is required. In the case of pigmented basal cell carcinoma, which can have some clinical features of a malignant melanoma, a punch biopsy is recommended because if the lesion proves to be a melanoma, recording the depth of the tumor is essential.\nIn addition, if a basal cell carcinoma is clinically suspected, but not found with a shave biopsy, a punch biopsy may be helpful in establishing a diagnosis, especially when infiltrative and morpheaform types of basal cell carcinoma are suspected. Because these tumors rarely metastasize, additional laboratory and imaging studies are not commonly indicated unless involvement of deeper structures, such as bone, is clinically suspected, in which case CT or radiography can be used.\n\n ## Figures\n\n \n*Page 3 of 5*",
"pagination": {
"current_page": 3,
"total_pages": 5
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914306,
"choiceText": "Morpheaform",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914307,
"choiceText": "Superficial",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914308,
"choiceText": "Nodular",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914309,
"choiceText": "Infiltrative",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 4,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 619935,
"questionText": "What is the most common type of basal cell carcinoma?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Lesions on a 51-Year-Old Man With Eyelid Cyst"
},
{
"authors": "Robert S. Bader, MD",
"content": [
"Because these tumors require supporting stroma for survival, metastasis is extremely rare and occurs in less than 0.55% of cases. As such, additional laboratory and imaging studies, beyond biopsy examination, are not commonly indicated unless involvement of deeper structures is suspected.",
"Treatment must be individualized for each lesion, with consideration of the histologic subtype of basal cell carcinoma, size, and site, and the age and sex of the patient. No single treatment is ideal for all types of basal cell carcinoma or for all patients. The goal of treatment is permanent cure with the best possible cosmetic result. Other factors, such as treatment cost, patient compliance, and postoperative course, must be considered. Recurrences are usually seen within the first year after treatment, and a minimum 5-year follow-up is recommended, especially to evaluate for the development of new tumors, because the risk for a second basal cell carcinoma is high.[3]",
"In most cases, a surgical modality is used, although nonsurgical treatment options are available. Such techniques include the following:",
"Electrodesiccation and curettage: This is a commonly used modality that is highly effective for nodular and superficial basal cell carcinoma, with reported cure rates as high as 95%. This treatment results in a scar, which in cosmetically sensitive areas must be considered. This treatment is not recommended for recurrent, infiltrative, or morpheaform types of basal cell carcinoma. The resultant wound requires daily care, which must be considered before treatment. Treatment on the lower legs can result in ulcers that can take 3 months or longer to heal, especially for larger or deep tumors.",
"Surgical excision: This is a commonly used treatment for most types of basal cell carcinoma. Frozen sections can be used for intraoperative margin control before closure. The tissue is processed with a bread-loafing technique, in which less than 1% of the margins are evaluated. Cure rates for nodular basal cell carcinoma have been reported to be 70%-95%.",
"Mohs micrographically controlled surgery: This has the highest cure rate for basal cell carcinoma. The surgeon also acts as pathologist and interprets the pathology slides. Unlike routine excision, all of the margins are evaluated histologically. Cure rates for primary, nonrecurrent tumors are as high as 99%. This method is the treatment of choice for morpheaform basal cell carcinoma and should be considered for recurrent tumors, tumors in areas where tissue sparing is essential (ie, ears, nose, eyelids, the T-zone of the face), larger tumors, and young patients.",
"Cryosurgery: This can be considered for smaller tumors.",
"Topical therapy: The best-studied treatment is imiquimod, which has a cure rate of approximately 80%. 5-Fluorouracil can also be effective. Monitoring is indicated, as recurrences are not uncommon.[6]",
"Photodynamic therapy: This has emerged as a treatment option for basal cell carcinoma, especially the superficial type.[7,8]",
"Ionizing radiation: This has long been known to be effective for the treatment of basal cell carcinoma, with cure rates as high as 97%. Various methods of delivery are used that may reduce the total number of treatment sessions required. In general, radiation is considered for older patients, many of whom are not good surgical candidates.",
"Several oral agents have been approved by the US Food and Drug Administration for use in locally advanced and metastatic basal cell carcinoma.[9] Vismodegib and sonidegib, hedgehog inhibitors, are approved for advanced or metastatic basal cell carcinoma recurrence following surgery or radiation therapy and for those who are not candidates for surgery or radiotherapy. Cemiplimab, a human monoclonal antibody PD-1 inhibitor, is approved for advanced or metastatic basal cell carcinoma that cannot be surgically removed or has progressed despite other treatments (eg, hedgehog inhibitors)."
],
"date": "February 04, 2025",
"figures": [],
"markdown": "# Lesions on a 51-Year-Old Man With Eyelid Cyst\n\n **Authors:** Robert S. Bader, MD \n **Date:** February 04, 2025\n\n ## Content\n\n Because these tumors require supporting stroma for survival, metastasis is extremely rare and occurs in less than 0.55% of cases. As such, additional laboratory and imaging studies, beyond biopsy examination, are not commonly indicated unless involvement of deeper structures is suspected.\nTreatment must be individualized for each lesion, with consideration of the histologic subtype of basal cell carcinoma, size, and site, and the age and sex of the patient. No single treatment is ideal for all types of basal cell carcinoma or for all patients. The goal of treatment is permanent cure with the best possible cosmetic result. Other factors, such as treatment cost, patient compliance, and postoperative course, must be considered. Recurrences are usually seen within the first year after treatment, and a minimum 5-year follow-up is recommended, especially to evaluate for the development of new tumors, because the risk for a second basal cell carcinoma is high.[3]\nIn most cases, a surgical modality is used, although nonsurgical treatment options are available. Such techniques include the following:\nElectrodesiccation and curettage: This is a commonly used modality that is highly effective for nodular and superficial basal cell carcinoma, with reported cure rates as high as 95%. This treatment results in a scar, which in cosmetically sensitive areas must be considered. This treatment is not recommended for recurrent, infiltrative, or morpheaform types of basal cell carcinoma. The resultant wound requires daily care, which must be considered before treatment. Treatment on the lower legs can result in ulcers that can take 3 months or longer to heal, especially for larger or deep tumors.\nSurgical excision: This is a commonly used treatment for most types of basal cell carcinoma. Frozen sections can be used for intraoperative margin control before closure. The tissue is processed with a bread-loafing technique, in which less than 1% of the margins are evaluated. Cure rates for nodular basal cell carcinoma have been reported to be 70%-95%.\nMohs micrographically controlled surgery: This has the highest cure rate for basal cell carcinoma. The surgeon also acts as pathologist and interprets the pathology slides. Unlike routine excision, all of the margins are evaluated histologically. Cure rates for primary, nonrecurrent tumors are as high as 99%. This method is the treatment of choice for morpheaform basal cell carcinoma and should be considered for recurrent tumors, tumors in areas where tissue sparing is essential (ie, ears, nose, eyelids, the T-zone of the face), larger tumors, and young patients.\nCryosurgery: This can be considered for smaller tumors.\nTopical therapy: The best-studied treatment is imiquimod, which has a cure rate of approximately 80%. 5-Fluorouracil can also be effective. Monitoring is indicated, as recurrences are not uncommon.[6]\nPhotodynamic therapy: This has emerged as a treatment option for basal cell carcinoma, especially the superficial type.[7,8]\nIonizing radiation: This has long been known to be effective for the treatment of basal cell carcinoma, with cure rates as high as 97%. Various methods of delivery are used that may reduce the total number of treatment sessions required. In general, radiation is considered for older patients, many of whom are not good surgical candidates.\nSeveral oral agents have been approved by the US Food and Drug Administration for use in locally advanced and metastatic basal cell carcinoma.[9] Vismodegib and sonidegib, hedgehog inhibitors, are approved for advanced or metastatic basal cell carcinoma recurrence following surgery or radiation therapy and for those who are not candidates for surgery or radiotherapy. Cemiplimab, a human monoclonal antibody PD-1 inhibitor, is approved for advanced or metastatic basal cell carcinoma that cannot be surgically removed or has progressed despite other treatments (eg, hedgehog inhibitors).\n\n ## Figures\n\n \n*Page 4 of 5*",
"pagination": {
"current_page": 4,
"total_pages": 5
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914310,
"choiceText": "Immunosuppression is a significant risk factor for metastasis.",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914311,
"choiceText": "Intravascular and perineural basal cell carcinomas are risk factors for metastasis.",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914312,
"choiceText": "Metastasis occurs more frequently in females vs males.",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914313,
"choiceText": "Skin is the most common site of metastasis, followed by regional lymph nodes, lung, bone, liver, and pleura.",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 5,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 619936,
"questionText": "Which of the following is most accurate regarding basal cell carcinoma metastasis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Lesions on a 51-Year-Old Man With Eyelid Cyst"
},
{
"authors": "Robert S. Bader, MD",
"content": [],
"date": "February 04, 2025",
"figures": [],
"markdown": "# Lesions on a 51-Year-Old Man With Eyelid Cyst\n\n **Authors:** Robert S. Bader, MD \n **Date:** February 04, 2025\n\n ## Content\n\n \n\n ## Figures\n\n \n*Page 5 of 5*",
"pagination": {
"current_page": 5,
"total_pages": 5
},
"questionnaire": [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 785887,
"choiceText": "Topical imiquimod",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785889,
"choiceText": "Topical 5-fluorouracil",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785891,
"choiceText": "Electrodesiccation and curettage",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785893,
"choiceText": "Vismodegib",
"correct": true,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Vismodegib is taken orally and may be used in the rare instance of metastatic basal cell carcinoma or for the treatment of locally advanced disease when other options are not feasible, similar to sonidegib (another hedgehog inhibitor) and cemiplimab (PD-1 inhibitor). Of note, pembrolizumab (PD-1 inhibitor) is used off-label in basal cell carcinoma that has progressed despite other treatments, such as hedgehog inhibitors.<br><br>\r\nIn this case, all of the above options were discussed with the patient in addition to excision. Electrodesiccation and curettage was chosen and performed without complication.",
"displayOrder": 2,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 246241,
"questionText": "Which treatment option would not be considered to treat a small, solitary superficial basal cell carcinoma?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 785895,
"choiceText": "Infiltrative basal cell carcinoma",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785897,
"choiceText": "Morpheaform basal cell carcinoma",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785899,
"choiceText": "Recurrent basal cell carcinoma",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785901,
"choiceText": "All of the above",
"correct": true,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Using local anesthesia, the surgeon removes the tumor along with a very thin layer of normal-appearing tissue around it. This layer is inked for orientation purposes and processed to make histopathologic slides for the surgeon to interpret. This method is the only one that evaluates all of the margins, thus sparing the greatest amount of normal, uninvolved skin. Cure rates for primary untreated basal cell carcinoma are greater than 99%. It is the treatment of choice for morpheaform basal cell carcinoma and is recommended for the treatment of infiltrative and recurrent basal cell carcinomas.",
"displayOrder": 3,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 246243,
"questionText": "Mohs micrographic surgery is an appropriate treatment for which of the following?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
],
"title": "Lesions on a 51-Year-Old Man With Eyelid Cyst"
}
] | [
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 785871,
"choiceText": "Nummular dermatitis",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785873,
"choiceText": "Pityriasis rosea",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785875,
"choiceText": "Superficial basal cell carcinoma",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785877,
"choiceText": "Guttate psoriasis",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 1,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 246237,
"questionText": "On the basis of the history, physical examination, and workup, what is the diagnosis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914306,
"choiceText": "Morpheaform",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914307,
"choiceText": "Superficial",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914308,
"choiceText": "Nodular",
"correct": true,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914309,
"choiceText": "Infiltrative",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 4,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 619935,
"questionText": "What is the most common type of basal cell carcinoma?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 1914310,
"choiceText": "Immunosuppression is a significant risk factor for metastasis.",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914311,
"choiceText": "Intravascular and perineural basal cell carcinomas are risk factors for metastasis.",
"correct": true,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914312,
"choiceText": "Metastasis occurs more frequently in females vs males.",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 1914313,
"choiceText": "Skin is the most common site of metastasis, followed by regional lymph nodes, lung, bone, liver, and pleura.",
"correct": false,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "",
"displayOrder": 5,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 619936,
"questionText": "Which of the following is most accurate regarding basal cell carcinoma metastasis?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 785887,
"choiceText": "Topical imiquimod",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785889,
"choiceText": "Topical 5-fluorouracil",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785891,
"choiceText": "Electrodesiccation and curettage",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785893,
"choiceText": "Vismodegib",
"correct": true,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Vismodegib is taken orally and may be used in the rare instance of metastatic basal cell carcinoma or for the treatment of locally advanced disease when other options are not feasible, similar to sonidegib (another hedgehog inhibitor) and cemiplimab (PD-1 inhibitor). Of note, pembrolizumab (PD-1 inhibitor) is used off-label in basal cell carcinoma that has progressed despite other treatments, such as hedgehog inhibitors.<br><br>\r\nIn this case, all of the above options were discussed with the patient in addition to excision. Electrodesiccation and curettage was chosen and performed without complication.",
"displayOrder": 2,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 246241,
"questionText": "Which treatment option would not be considered to treat a small, solitary superficial basal cell carcinoma?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
},
{
"answered": false,
"answeredCorrectly": false,
"branch": false,
"choices": [
{
"branchPath": null,
"choiceId": 785895,
"choiceText": "Infiltrative basal cell carcinoma",
"correct": false,
"displayOrder": 1,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785897,
"choiceText": "Morpheaform basal cell carcinoma",
"correct": false,
"displayOrder": 2,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785899,
"choiceText": "Recurrent basal cell carcinoma",
"correct": false,
"displayOrder": 3,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
},
{
"branchPath": null,
"choiceId": 785901,
"choiceText": "All of the above",
"correct": true,
"displayOrder": 4,
"explanation": "",
"hideLabel": false,
"selected": false,
"totalAbsoluteResponseCount": 0,
"totalResponses": "0"
}
],
"discussion": "Using local anesthesia, the surgeon removes the tumor along with a very thin layer of normal-appearing tissue around it. This layer is inked for orientation purposes and processed to make histopathologic slides for the surgeon to interpret. This method is the only one that evaluates all of the margins, thus sparing the greatest amount of normal, uninvolved skin. Cure rates for primary untreated basal cell carcinoma are greater than 99%. It is the treatment of choice for morpheaform basal cell carcinoma and is recommended for the treatment of infiltrative and recurrent basal cell carcinomas.",
"displayOrder": 3,
"displayType": 1,
"horizontal": false,
"introduction": "",
"matrixQuestions": [],
"mutuallyExclusive": false,
"poll": true,
"professions": [],
"questionId": 246243,
"questionText": "Mohs micrographic surgery is an appropriate treatment for which of the following?",
"questionTypeId": 1,
"required": false,
"responseText": null,
"score": false,
"showAnsTable": true,
"showQuestion": true,
"showResult": true,
"specialties": [],
"totalResponses": 0,
"viewResults": false
}
] |
831467 | /viewarticle/831467 | [{"authors":"Lars Grimm, MD, MHS; Malkeet Gupta, MS, MD; Rick G. Kulkarni, MD","content":["Editor'(...TRUNCATED) | [{"answered":false,"answeredCorrectly":false,"branch":false,"choices":[{"branchPath":null,"choiceId"(...TRUNCATED) |
731857 | /viewarticle/731857 | [{"authors":"Andrew Melone, MD; David F. Baehren, MD","content":["Editor's Note:\nThe the Case Chal(...TRUNCATED) | [{"answered":false,"answeredCorrectly":false,"branch":false,"choices":[{"branchPath":null,"choiceId"(...TRUNCATED) |
832278 | /viewarticle/832278 | [{"authors":"Jansen Tiongson, MD; John Sakles, MD; Harvey W. Meislin, MD","content":["Editor's Not(...TRUNCATED) | [{"answered":false,"answeredCorrectly":false,"branch":false,"choices":[{"branchPath":null,"choiceId"(...TRUNCATED) |
1002140 | /viewarticle/1002140 | [{"authors":"D. Brady Pregerson, MD","content":["Editor's Note: The Case Challenge series includes d(...TRUNCATED) | [{"answered":false,"answeredCorrectly":false,"branch":false,"choices":[{"branchPath":null,"choiceId"(...TRUNCATED) |
738325 | /viewarticle/738325 | [{"authors":"Nirupam Prakash, MD, MBBS","content":["Editor's Note:\nThe Case Challenge series includ(...TRUNCATED) | [{"answered":false,"answeredCorrectly":false,"branch":false,"choices":[{"branchPath":null,"choiceId"(...TRUNCATED) |
833922 | /viewarticle/833922 | [{"authors":"D. Brady Pregerson, MD","content":["Editor's Note:\nThe Case Challenge series includes (...TRUNCATED) | [{"answered":false,"answeredCorrectly":false,"branch":false,"choices":[{"branchPath":null,"choiceId"(...TRUNCATED) |
922415 | /viewarticle/922415 | [{"authors":"Sarah Taber, MD","content":["Editor's Note: The Case Challenge series includes difficul(...TRUNCATED) | [{"answered":false,"answeredCorrectly":false,"branch":false,"choices":[{"branchPath":null,"choiceId"(...TRUNCATED) |
End of preview. Expand
in Dataset Viewer.
Explore data
Articles and Pages Format.
article_id: id of article.
url: path to article https://reference.medscape.com/{view article path}
article_data: Store all pages in article. Each page will store content of medical cases (paragraphs, figures) and some related questions.
- title: title of page.
- authors: authors' name.
- date: posted date.
- content: list of paragraph text corpora.
- figures: a list of captions and image_url links for figures.
- pagination: information about pagination.
- questionnaire: related questions asked in this page.
- markdown: A condensed markdown version created from content field and figure field.
questions: a list of questions asked in article_data (the same "questionnaire" field in article_data).
Questions Format
- questionId: id of question.
- questionText: Question text shown for user.
- ...
- choices: a list of choices
- choiceText: choice text shown for user.
- choiceId: id of choice.
- correct: true / false, true means this choice is the answer to question otherwise it is not.
- ...
- Downloads last month
- 9